Infant PPI Dosing Information

PPI Dosing information and dosing chart for suggested doses of PPI drugs (proton pumps inhibitors) and the treatment of infant acid reflux. A guide to help you choose the right PPI dose for your child whether you are using TummyCare Max® or any other infant acid reflux treatment options.
Did you know that your baby, or any infant and child, metabolize most medications at a much faster rate then adults? Sometimes up to three times faster. The dosing recommendations below are what many medical doctors and researchers have been studying and applying "SUCCESSFULLY" for the past fifteen years. As you can see in the chart below (the metabolism of a drug can be measured as half-life) the half-life of lansoprazole for an infant is much shorter than for an adult. This is true for all the PPIs.
The PPI dosing information on this page is an important reference and tool, and if you decide to use this treatment regimen as part of your baby's acid reflux treatment and you can apply it regardless of the PPI drugs you currently use. In addition we offer this information to you whether you've decided to use our infant acid reflux buffer product TummyCare Max®, or if you've chosen an alternative acid reflux treatment option.
We'd also like to point out that we always stress the importance reviewing and discussing all infant acid reflux treatment intentions with your doctor and we encourage you to refer anybody in your care provider team to review this website and this page.
PPI Dosing Information. Dosing Regimen:
The use of all medicines in both children and adults is simply the combination of a dose (the quantity in which the PPI drug is given) and a dosage interval (the multiple of times the PPI drug given). This combination makes up the drug regimen. Most of the drug regimens that are used in children are based on adult information. For example, a common drug regimen for adult suffering from acid reflux in the esophagus would be Prevacid® (lansoprazole) 30mg twice per day. In this case the dose is 30mg and the dosage interval is twice per day. The adult PPI dosing information is important because we rarely have specific PPI dosing information for children. This is due to the difficulty in doing clinical testing on infants and children.
PPI Drugs. How Much Is Enough?
Note that each of the listed PPI drugs below are currently approved by the FDA for pediatric use.
- Esomeprazole, found in Nexium®
- Omeprazole, Prilosec®, Zegerid®
- Lansoprazole, found in Prevacid® and generic forms
- Pantoprazole, found in Protonix®
PPI drugs have an effect on the production of acid. That effect is related to the amount of drug that is absorbed into the body. This amount of drug is known as the AUC or Area Under the Curve. So, when planning out a drug regimen with a PPI drug, the best thing to do is to try to achieve an AUC that is known to inhibit enough acid in twenty four hours to reduce damage and reduce symptoms. In other words, you have to give enough quantity of the PPI drugs and frequently enough to get the desired effect.
When the dosing level of the PPI drug is too low, the child will continue to suffer from the acid reflux and the symptoms may be misdiagnosed. This could contribute to the assumption that PPI drugs do not have an effect on infants. This is also the primary cause of what is commonly referred to as the acid battle.
The natural concern is whether you can over dose (give too much) PPI medication to your baby?
The short answer is no.
PPI's are very specific in where they work in the body. They are only active in a very specific place and that is the acid secreting portion of a cell called parietal cell. Since PPI drugs only work on the acid secreting cell the chance of side effects is very, very low even if you give three times more then your child needs. Additionally, PPI drugs are known as prodrugs because they are not active as they pass from the bloodstream to parietal cell. PPI's become active only when they pass into the acid secreting portion of the parietal cell. This is where the pH level drops to approximately one (1) pH, a safe pH level for the drug so it does not get destroyed.
Finding the correct drug regimen can be a challenge. Fortunately, this PPI dosing information page and the dosing chart will assist you in reaching the optimal dose for your baby based on the age and weight of your child. There are some variables and as your baby gets older and their weight changes, so will your drug regimen. Some infants or children just require a higher dose to control acid reflux symptoms so there may be times when you would want to increase the milligram (mg) per milliliter (mL) concentration. That is what this PPI Dosing information is here for. To act as a guide in optimizing, adjusting, and hopefully at one point weaning your baby off PPI drugs all together.
Remember that a drug regimen is made up of a dose and a dosage interval. We discussed that an adult might take Prevacid® (lansoprazole) 30mg twice per day. So the dose is 30mg and the interval is the twice per day. We need to calculate a dose and an interval for your child. Determining the drug regimen can be done in two ways:
- One way is to have your child take the medicine (such as lansoprazole or omeprazole) and then measurements of the drug in the bloodstream are taken. This process is called pharmacokinetics. From this measurement you will learn two primary pieces of information (we can call them pharmacokinetic variables, because they vary a little from person to person), the half life (t1/2) and the volume of the distribution (Vd).
Half life is time required for the drug concentration in the bloodstream to drop by ½. It is used to determine the dosage interval (number of doses per day) and is measured in minutes or hours.
Volume of distribution relates to how the drug moves into the tissues of the body. It is used to determine the dosage and is measured in L/kg.
Thankfully you can approach the second option below which is a much easier. Just follow the steps of the PPI dosing information page as indicated below.
- The easiest way to determine the correct drug regimen for your child is to find a study that has already evaluated the pharmacokinetics of children and reported the half-life and the volume of distribution for various weights and ages of children.
The Marci-kids website used to provide this information and we have it archived here on www.infant-acid-reflux-solutions.com. The PPI dosing information chart is based on the evaluated pharmacokinetics studies and have been converted into a drug regimen table by Dr. Jeffrey Phillips, the head research in the department of surgery at the University of Missouri and Dr. Marcella Bothwell (Marci), ENT Rady Children's Hospital in San Diego, CA. A twelve year study that both Dr. Jeffrey Phillips and Dr. Marcella Bothwell successfully used to treat hundreds or infants and children using this drug regimen.
Determining a drug regimen this way is much easier since you don't have to get blood draws from your child after they have taken a dose of the medicine.
Let's start with an example of calculating the half-life to tell us the number of doses per day. The average adult with acid reflux disease takes a PPI drug once to two times a day. This can act as our baseline for the number of doses per day. Now compare how the half-life of children differs from adults and modify the number of doses per day accordingly
- Find the child's age at the bottom of the graph.
- Draw a line straight up until your intersect the slanted line drawn on the graph.
- Plot over to the left where you see the half-life in hours.
- The example shows a one year old infant taking lansoprazole (see red arrows).
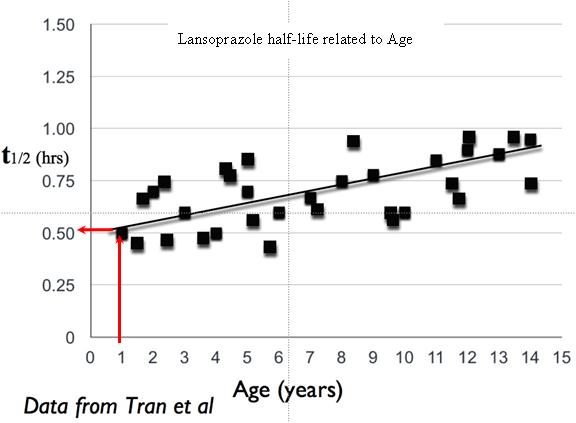
Tran A, Rey E, Pons G, Pariente-Khayat A, d'Athis P, Sallerin V, Dupont C. Pharmacokinetic-pharmacodynamic study of oral lansoprazole in children. Clinical Pharmacology and Therapeutics. 2002;71: 359-367.
Based on this process indicated on this PPI dosing information page, the estimated half-life for this child would be 0.5 hours. Published data indicates that the normal adult has half-life of 1.5 hours for lansoprazole. By dividing the adult half-life of 1.5 hours by this child's half-life of 0.5 hours (as indicated on the table above), we know this child would estimate the lansoprazole three times faster then the adult.
The average adult takes 1 dose per day (baseline from above) to achieve good acid control, so this one year old would be expected to need 3 doses per day (3 x 1). Now we know that this child will need 3 doses per day.
Now lets calculate the dose. The amount of PPI is determined by multiplying the volume of distribution and the child's weight. For lansoprazole and omeprazole, research has shown that the Vd (volume of distribution) is 3 to 4 times larger in children than in adults. The average adult dose is approximately 0.5 mg/kg therefore,
3 x 0.5 mg/kg = 1.5 mg/kg per dose and
4 x 0.5 mg/kg = 2 mg/kg per dose
Because some infants or children just require a higher dose to control acid reflux symptoms so there may be times when you would want to increase the milligram (mg) per milliliter (mL) concentration.
If you begin using a compounded suspension or any of our infant acid reflux buffer products following the guidelines below, and you are not seeing satisfactory results (significant or complete relief from the acid reflux) a higher dose might be required. This might be accomplished by giving your baby a little more (one or two milliliters) of the suspension at each dosing time. Or if your baby is experiencing excess gas it may be useful to mix the suspension at a higher mg per ml concentration.
It is generally a good idea to wait seven to ten days before making any additional adjustments as it could take this long for the PPI drugs to have their full effect.
Let's begin. Choose the dose that is recommended for your baby's age and multiply the milligrams per pound of body weight as indicated in the charts. Then administer that dose as many times as recommended on the chart above.
PPI Dosing Information Charts:
Lansoprazole Lansoprazole (Prevacid®) is typically mixed at a 3mg per ml concentration.
| Childs; Age | Doses; per pound of body weight | Doses; per day; |
| Under 3 months old | 0.7mg to 0.8mg of PPI per pound of body weight | 3 times per day |
| 3 to 6 months old | 0.6mg to 0.7mg of PPI per pound of body weight | 3 times per day |
| 7 months to 2 years old | 0.45mg to 0.6mg of PPI per pound of body weight | 3 times per day |
| 2 years old or older | 0.45mg of PPI per pound of body weight | 2 to3 times per day |
| 5 years old or older | 0.35mg to 0.45mg of PPI per pound of body weight | 2 times per day |
Omeprazole (Prilosec®, Zegerid® and generic forms) and Esomeprazole (Nexium®) All other PPI drugs (Nexium®, Prilosec®, Zegerid® as well as the generic versions of Omeprazole) are typically mixed at a 2mg per ml concentration.
| Childs; Age | Doses per pound of body weight | Doses; per day; |
| Under 3 months old | 0.7mg of PPI per pound of body weight | 3 times per day |
| 3 to 6 months old | 0.6mg of PPI per pound of body weight | 3 times per day |
| 7 months to 2 years old | 0.45mg of PPI per pound of body weight | 3 times per day |
| 2 years old or older | 0.45mg of PPI per pound of body weight | 2 to 3 times per day |
| 5 years old or older | 0.35mg of PPI per pound of body weight | 2 times per day |
PPI Dosing Information - Titrating Up or (Weaning Up)
The acid in the stomach is very high in concentration when starting a proton pump inhibitor medication and a drug regimen. This of course is what's causing the infant acid reflux symptoms. It also causes the biggest difficulty when beginning your infants drug regimen. This is called "The Acid Battle" and we get into great detail about this subject on "The Acid Battle" page.
We also go into detail about how to wean or titrate your baby up or down from proton pump inhibitors so assist in the process and making the dosing up process as smooth as possible. Please read about it here on the Weaning page.
PPI Dosing Information for Pharmacy Compounds
If you are currently giving your child a compounded suspension of a PPI such as Prevacid® made by a pharmacy, you should know that there is a good potential for the medication to become inactive (and therefore ineffective) in a much shorter time period than your pharmacist may be aware. The loss of activity is related to the effect of the flavorings added by the pharmacies. Some of the flavorings may cause the PPI to become unstable and break down so it can no longer inhibit acid secretion.
In addition, many pharmacies do not add enough buffer in their suspensions to protect the drug from degradation by stomach acid. This is particularly a problem if the child is receiving a very low-volume dose (less than 3 ml, for example) because the amount of buffer most likely will not be enough to protect the PPI from degradation by stomach acid.
The Harriet Lane Handbook, a trusted source of pediatric PPI dosing information for more then fifty years also states, "The extemporaneously compounded oral suspension product MAY BE LESS BIOAVAILABLE owing to the loss of the enteric coating."
John Hopkins: The Harriet Lane Pediatric Handbook 17th ed., Copyright© 2005 Mosby.
Note: The doses recommended on our PPI dosing information page as well as in the dosing chart are not recommended or discouraged by any proton pump inhibitor manufacturer or distribution company.
we want to hear from you!
Tell us your story and pay it forward by sharing your experiences. Our customer reviews are important to us and to the Mom's, Dad's caring for babies suffering from infant acid reflux.
*MBCHB, FRCPC, FACG. Decisions in diagnosing and managing chronic gastroesophageal reflux disease in children. Journal of Pediatrics 2005; 146:3-12
Burnett JE, Balkin ER. Stability and viscosity of a flavored omeprazole oral suspension for pediatric use.
American Journal of Health-Systems Pharmacy 2006; 63:2240-2247.
Clinical studies showing that higher PPI doses are required to achieve healing in pediatric patients are listed here on the PPI dosing information page below. Along with them are the credits for those who participated and published these studies:
Gunasekaran TS, Efficacy and safety of omeprazole for severe gastroesophageal reflux in children. The Journal of Pediatrics 1993; 123:148-154.
Israel D, Shepherd R, et al. Omeprazole for treatment of chronic erosive esophagitis in children: a multi-center study of efficacy, safety, tolerability and dose requirements. The Journal of Pediatrics 2000; 137:800-807.
Iarocci TP, Tan H, Singer, J, Barron J, Pilzer E, Patel D, Bakst A. Proton pump inhibitors in infants. [Abstract] American Journal of Gastroenterology. 2005; 100(suppl.):S273.
Clinical study of pharmacokinetics of omeprazole in children
Andersson T, Lundborg P, et al. Pharmacokinetics of orally administered omeprazole in children. American Journal of Gastroenterology 2000; 95:3101-3106.
Pharmacokinetic study showing the relationship between lower age and higher dosing requirements in pediatric patients: younger children require higher and/or more frequent doses due to shorter PPI half-life. The first author is employed at Astra (company that makes Prilosec.)
Reviews of PPI use in children: pharmacokinetics, safety, efficacy, and PPI dosing information
Israel DM, Omeprazole and other proton pump inhibitors: pharmacology, efficacy, safety, with special reference to use in children. Journal of Pediatric Gastroenterology and Nutrition. 1998; 27:568-579.
Specifically states that on a per kilogram (weight) basis, children require higher doses of omeprazole than adults due to different pharmacokinetics of omeprazole in children. Discusses at length the use of buffered PPI suspensions in children as a preferred dosage form.
Litalien C, Theoret Y, Faure C. Pharmacokinetics of proton pump inhibitors in children. Clinical Pharmacokinetics 2005; 44:441-466.
Abstracts by Jeffrey Phillips, Pharm.D., describing use of ChocoBase and CaraCream in pediatric patients; includes some PPI dosing information
Phillips JO, Bettag ME, Parsons DS, Wilder B, Metzler MH. Use of flavored lansoprazole or omeprazole suspensions in pediatric GERD. [Abstract A1292] Gastroenterology 2000; 118: 5904.
Phillips JO, Parsons DS, Fitts SW. Flavored lansoprazole suspension in pediatric GERD. [Abstract] Journal of Pediatric Gastroenterology and Nutrition 2000; 31:S181. [Abstract No. 707].
This PPI dosing information and chart and a portion of the textual contents of the PPI dosing information page came from the Marci-kids website.